Cervical, Mediastinal, Intraspinal and Paraaortic Emphysema Secondary to Asthma Exacerbation Case Report-Juniper Publishers
Juniper Publishers-Journal of Pediatrics
Abstract
Cervical and mediastinal emphysema associated with
acute asthma exacerbation is very rare. In most cases, air leakage from
ruptured alveolar escapes and dissects the hilum along
peribronchovascular sheaths and spreads to mediastinum. Once in the
mediastinum, air extends around the large vessel and esophagus to
thoracic wall. This report presents the case of 3 years old patient with
background of asthma who presented to the emergency room with palpable
cervical emphysema, wheezy chest and CT evidence of cervical and
mediastinal emphysema. There are only a limited number of case reports
associated with cervical and mediastinal emphysema in the absence of
pneumothorax in patient with asthma.. To our knowledge, this maybe the
first report in pediatric where cervical, mediastinal, intraaspinal and
paraaortic emphysema is induced by asthma exacerbation in the
literatures.
Keywords:Asthma; Emphysema; PediatricIntroduction
Cervical and mediastinal emphysema associated with
acute asthma exacerbation is rare. This report presents 3-years old boy
with recurrent asthma who presented with clinical significant cervical
emphysema. Only limited number of cases have been reported with cervical
and mediastinal emphysema in the absence of pneumothorax in patients
with asthma.
Case Presentation
A 3 years old boy presented to our emergency
department with cough, fever, shortness of breath, vomiting, muffled
voice and throat pain for 2 days. He had history of recurrent chest
wheezing attacks that were controlled by salbutamol nebulization. There
was no history of contact with sick patients or animal pets. The child
was fully vaccinated. He had manifest distress and his oxygen saturation
on room air was 95%. His temperature was 38.5 °C, respiratory rate was
58per/min and heart rate=125/min. The Neck was swollen with crackling
sensation due to subcutaneous emphysema. Sub costal and inter costal
retraction was evident. On auscultation there was bilateral wheeze heard
all over the chest. He was started on 5 L oxygen, salbutamol Nebulizer.
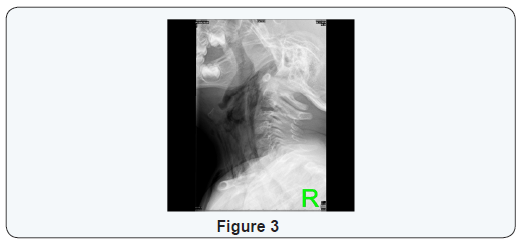
Lateral neck radiography showed increased thickness
in the nasopharyngeal region and narrowing in the nasopharyngeal air
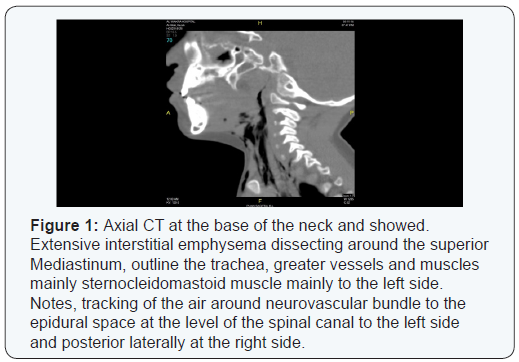
column. CT scan of the neck revealed extensive air in the
retropharyngeal space extending to the subcutaneous tissue of the neck,
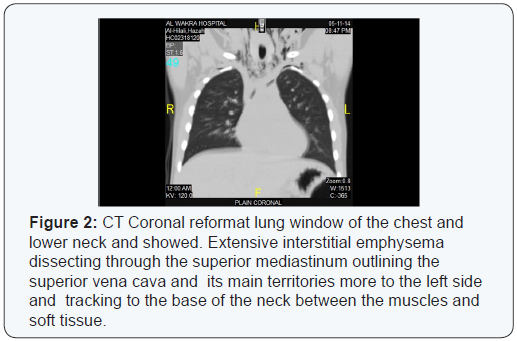
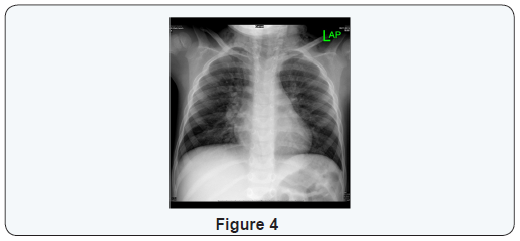
mediastinum and interaspinal canal. CT chest shows some air noted
surrounding the aorta at the D 12 level. The lung parenchyma showed
exaggerated broncho-vascular markings and mild septal thickening. The
patient was shifted to pediatric ICU where he was started on high flow
oxygen, intravenous antibiotics and continued on salbutamol nebulizer.
Within 3 days of hospital admission he showed dramatic clinical and
radiological improvement.
Discussion
Cervical and mid mediastinal emphysema may occur
secondary to bronchial asthma, retropharyngeal abscess or lateral space
abscess. Pneumo-mediastinum (PM) usually results from the over
distension of the alveoli, with rupture, allowing air to enter
interstitial tissues and extend into the mediastinum, neck, or
intrathoracic areas. Wong et al. [1] analyzed 87 children with
spontaneous pneumothorax. Forty-three patients (49.4%) had a primary
idiopathic spontaneous pneumothorax (SPM). The most common cause of
secondary SPM was bronchial asthma with an acute exacerbation. None of
the patients <6 years (n=16) had primary PM while 60% of patients
>6 years had primary PM (0% vs 60%) Therefore, a high index of
suspicion for underlying causes
of SPM should always be kept in mind for young children younger
than 6 years [1].
Bronchial asthma predisposes to the development of
SPM [2] because asthma augments airway epithelial injury
and increases alveolar rupture due to lung hyperinflation
[1]. Pneumomediastinum is defined as the presence of free
air in the mediastinum. It can be divided into spontaneous
pneumomediastinum (SPM) (without any obvious primary
source) and secondary or traumatic pneumomediastinum due to
a mediastinal organ injury caused by trauma, surgery or medical
procedures. According to Macklin’s experimental animal model,
alveolar rupture leads to air infiltration along the bronchovascular
sheath with free air finally reaching the mediastinum. Furthermore,
if the air travels along tissue planes it can reach the neck, face,
abdomen or even the limbs, leading to subcutaneous emphysema
[3].
SPM was originally described by Louis Hamman in 1939 (34),
while later it was identified as Hamman’s syndrome. Sudden onset
of symptoms of SPM include retrosternal pain (80%), rhinophonia
and/or hoarseness (65%), dyspnea (46%), cough (26-45%),
subcutaneous emphysema (32%), sore throat (18%), and neck
pain (4-38%) (43). According to several reports, the most common
presenting complaints are chest pain, shortness of breath and
subcutaneous emphysema. The diagnosis of pneumomediastinum
is based upon radiographic examination. CT chest scan is a better
means of diagnosis compared to plain chest X-ray film [4].
Management of Pneumomediastinum depends upon
whether or not it is complicated. Uncomplicated SPM is managed
conservatively with analgesia, rest, and avoidance of maneuvers
that increase pulmonary pressure (Valsalva or forced expiration,
including spirometry). Therapy with high concentration oxygen
has been used in an effort to enhance nitrogen washout, but is
probably not necessary except in patients with severe symptoms.
If such patients have underlying chronic lung or airway disease
that predisposes to atelectasis, 100 percent oxygen therapy should
be administered with caution, because it may lead to absorptive
atelectasis [5].
Massive pneumomediastinum may be complicated by tension
pneumomediastinum, which may interfere with breathing or
venous return. In this case, limited mediastinotomy may be
performed to drain the pneumomediastinum [5]. The outcome
of SPM is usually good and this benign condition usually resolves
without consequences within 2 to 15 days, often after a transient
worsening of symptoms. Recurrent SPM occurs in less than 5
percent of cases, and such recurrences are typically also benign
[6].
Learning Points
Although cervical and pneumomediastinum is a rare
complication of asthma in pediatric age group, specially
those who are less than 6 years, it should be considered
always in the differential diagnosis. The clinical presentation of pneumomediastinum secondary to asthma exacerbation
varies widely, so imaging study, including CT scan and X-ray are
recommended to narrow the differential diagnosis. Supportive
measurement is a treatment modality in most of the cases, but
surgical intervention is needed in some of the cases (Figure 1 to
4).
For more articles in Academic Journal of
Pediatrics & Neonatology please click on:
https://juniperpublishers.com/ajpn/index.php
https://juniperpublishers.com/ajpn/index.php


Comments
Post a Comment