Complete Transection of Right Bronchus in Blunt Trauma of Chest _ A Rare Finding-Juniper Publishers
Juniper Publishers-Journal of Pediatrics
Abstract
Tracheo-bronchial disruption is one of the less common injuries associated with blunt trauma chest in children. This injury can be life threatening. Failure to diagnose it early can lead to disastrous acute or delayed complications. This can be easily overlooked on initial evaluation in the emergency room (ER) as the focus of the attending physician is diverted to more obvious external injuries which may not be of much significance. Herewith we present a case of a 3 year old female child, who was admitted via our emergency room (ER) with a reported history of chest injury due to being run over by a rickshaw. She was conscious and presented with chest pain and respiratory distress. Physical examination revealed surgical emphysema, but no clinical rib fracture. X-ray chest postero-anterior view showed pneumothorax and pneumomediastinum. A chest drain was surgically placed on her right side and there was profuse bubbling noted. Her oxygen saturation was decreasing continuously. So we then suspected some form of tracheal or bronchial injury and we emergently performed a thoracotomy in the ER. On opening the thorax, the right bronchus was transected at the carina and the remaining bronchus was crushed and devitalized. Additionally the Right lung sustained a contusion. It was not possible to primarily repair the right sided bronchus due to crush injury observed, so a pneumonectomy was performed on the right side and a chest drain placed. The child’s post-operative period was uneventful and the patient was discharged after 8 days. Transection of a bronchus due to blunt trauma is fortunately a very rare presentation, especially without any other significant associated injuries.Keywords:Blunt trauma chest; Bronchial transaction; Pneumonectomy
Introduction
Tracheo-bronchial disruption is one of less common
injuries associated with blunt trauma chest. This injury can be life
threatening, however, failure to diagnose it early can lead to
disastrous acute or delayed complications [1]. Bronchial transection has
a variety of clinical presentations due to massive air leak into the
pleural cavity and it is very rare to have a total absence of air leak
from a transected bronchus at presentation. Most commonly, the patient
will typically present with dyspnoea and varying degrees of respiratory
distress. These injuries are most commonly due to forceful trauma, such
as secondary to motor vehicle injuries.
Case Report
A 3 years old female child was admitted to our
emergency room (ER) with a history of chest injury due to a collision
with a rickshaw. The rickshaw reportedly ran over the young child’s
chest shortly before being rushed to our medical centre for care. The
child presented with acute chest pain and respiratory distress despite
remaining conscious and hemodynamically stable. Physical examination
revealed tenderness on the right side of her chest, no
clinical evidence of rib fracture, surgical emphysema or decreased chest
movements on the right side. On auscultation breath sounds were absent
on the right side and on percussion the right side was resonant. There
were no other associated injuries observed. A postero-anterior view
chest X-ray was performed, which showed pneumothorax and
pneumomediastinum. As such, a chest drain was emergently placed in her
right chest and there was a large amount of air noted. Profuse bubbling
was continued for more than 1hr and despite this her oxygen saturation
was decreasing continuously. So we suspected some form of tracheal or
bronchial injury and decided to perform an emergency room thoracotomy,
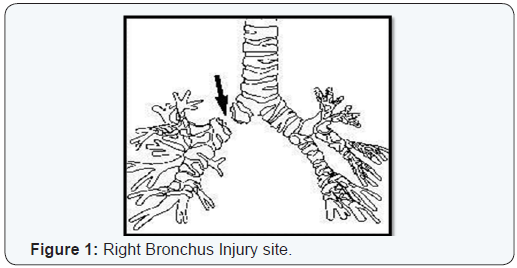
given her unstable and worsening status. When we opened the thorax, we
found that her right bronchus was transected at the carina (Figure 1)
and the remaining bronchus was crushed and devitalized. The right lung
was also notably contused. So it was not possible to perform a primary
repair of the bronchus on that side. We then performed a pneumonectomy
on her right side and placed a chest drain. The post-operative period
was uneventful and the patient was discharged after 8 days (Figure 2).

Discussion
An isolated total transaction of the bronchus due to blunt
trauma of the chest without any other associated injury is
highly unusual, yet a critically important consideration in
the early management of trauma patients not responding
appropriately to standard management. In our reported case,
there was no possibility of primary repair of bronchus, so a right
pneumonectomy was done. Tracheo-bronchial injury is defined as
any traumatic injury to the trachea or bronchi from the level of
the carotid cartilage to the division of the lobar bronchi into the
segmental branches. Although injuries to the tracheo-bronchial
tree are observed infrequently after blunt trauma, reports of
such injuries are not unheard of [2]. This condition demands
early recognition and prompt surgical therapy for a successful
outcome [3]. Signs and symptoms are non specific and can
include dyspnoea, desaturation, decreased breath sounds, hyperresonance,
tracheal shift and distended neck veins. Tracheal or
bronchial injuries should be suspected in patients with increasing
or persistent pneumothorax despite of continuous intercostal
tube drainage. Injury to the trachea or proximal bronchus
results typically in pneumomediatinum and not pneumothorax.
Possible mechanism for this type of injury may be due to either
compression of the bronchus between the sternum and vertebra
or due to a sudden increase in intrabronchial pressure at the time
of injury [4]. Laceration of the bronchus involving more than
one third of the circumference of the bronchus requires surgical
treatment and severely injured cases may need pneumonectomy
[5]. The outcome depends on the general condition of the
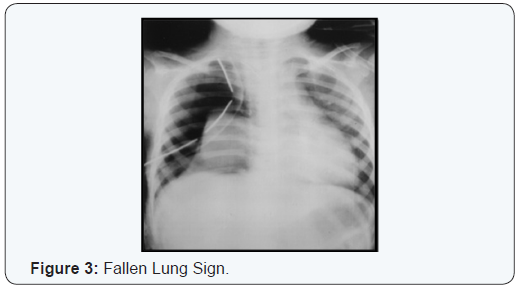
patient and also the associated injuries. The constellation of
persistent pneumothorax, massive air leak, and atelectatic
lung in the presence of a well placed, functional thoracostomy tube constitues the “fallen lung” sign (Figure 3) and is a chest
roentgenogram finding of high specificity for intrathoracic airway
rupture [1]. A pneumothorax is frequently present, but may be
absent if the mediastinal pleura remains intact. For the diagnosis,
bronchoscopy is the first method of choice [2]. It is reported that
three-dimentional helical computed tomography might be used in
the diagnosis as well [3].
Conclusion
- Tracheo-bronchial injuries are usually rare and transection of the tracheo-bronchial tree due to blunt trauma of the chest is even rarer.
- It is very rare to find total transaction of the right bronchus, in case of blunt trauma of chest without any other associated injury. Given the extensive injury sustained, we were unable to perform a primary repair of the bronchus, so a right pneumonectomy was performed emergently.
- Sign and symptoms are non specific. So high degree of suspicion is required to diagnose trachea-bronchial injuries.
- Immediate diagnoses and treatment is required for saving the life of the patient.
- A transected trachea or bronchus may successfully undergo end to end anastomosis, unless there is severe injury to the organs, in which case a pneumonectomy may be indicated, as in our case report.
For more articles in Academic Journal of
Pediatrics & Neonatology please click on:
https://juniperpublishers.com/ajpn/index.php
https://juniperpublishers.com/ajpn/index.php


Comments
Post a Comment